Denise Ann Edgar1, James Brinton1, Bernadette Burgess 1, Vanathy David1, Melissa Glass1 and Lynda Horning1
Abstract
Clinical Nurse and Midwifery Consultants (CNC/CMCs) play an important role within NSW Health Services. They are required to function within five domains of practice: clinical service and consultancy, clinical leadership, research, education, and clinical services planning and management. This study engaged with one Health District's current CNC/CMC network members with a view to informing the development of a strategy for career and succession planning. One hundred CNC/CMCs were invited to participate in an online survey and in one of three focus groups. The survey explored: the participants' demographics, their educational pathways prior to and during the role, the relationship of this education to the five domains of CNC/CMC practice, their priorities for their own future education needs, the education priorities they suggested for other aspiring CNC/CMCs, and who was mentoring into their role. The focus group added further clarity to the survey data. The survey was completed by 61% of invitees and 19% attended the focus groups. The findings identified an experienced workforce, with 25% of CNC/CMCs intending to leave over the next five years, yet only 20% mentoring others. Nearly half (47%) of the participants held or were working towards a Master's degree. A third of these Master's degrees were considered by the participants to support knowledge in all five of the CNC/CMCs' domains of practice, in comparison to only 11% of graduate certificates. The focus-group participants expressed the view that the Master's qualification supported them to meet the domains of the CNC/CMC role, and suggested that aspiring CNC/CMCs should aim for this level of education. When considering their own personal educational needs, the CNC/CMCs prioritised service planning and management and research, but they felt that aspiring CNC/CMCs should prioritise the development of clinical knowledge, followed by clinical leadership.
Keywords: clinical nurse consultant, clinical midwifery consultants,education preparation, succession and career planning
1 Illawarra Shoalhaven Local Health District
Corresponding author: Denise Edgar, Nurse Manager, Nursing and Midwifery Research Unit, Level 8, The Wollongong Hospital ISLHD, NSW, [email protected]
This study was conducted in one Local Health District (LHD) in NSW Australia that has a combined rural and regional status. The LHD comprises eight hospitals and 45 community-based service sites. It employs 3,500 nurses, including 95 permanent Clinical Nurse/Midwifery Consultants (CNC/CMCs). All CNC/CMCs belong to a CNC/CMC Network - a local professional body that meets regularly to discuss professional issues and to plan their collective requirements for supporting and enhancing these roles. A growing concern within the CNC/CMC Network was the age of its current members and the need for succession planning; this is a concern shared by the Nursing and Midwifery Executive (Walsh et al. 2015). The current District mentoring program provides support when new CNC/CMCs are appointed, but there is no formal program in place for aspiring CNC/CMCs.
A small group of diverse CNCs (n = 5) came together to enhance their research capabilities, research being a domain of the CNC role. This group agreed to find a research question that was of interest to the CNC/CMC Network and to the District's Nursing and Midwifery Leadership team. The topic of succession and career planning was discussed and the research team began to consider how it could be approached from a research perspective. It was apparent that a central repository of demographic information about the CNC/CMC Network as a collective was lacking, making it difficult to confirm or deny the CNC/CMCs' concerns.
The CNC/CMC role has been embedded in the fabric of NSW Health's nursing workforce since the 1980s, giving reward and recognition to expert nurses (Chiarella, Hardford & Lau 2007). The role encompasses five domains of practice: research, education, clinical leadership, clinical services and consultancy, and clinical service planning and management (NSW Ministry of Health 2017). However, in reality, these consultant roles are diverse and complex in nature (Bloomer & Cross 2011; Walsh et al. 2015) and are often enacted with large variability (Roche et al. 2013; Walsh et al. 2015). A number of factors can account for this diversity. First, the role has been divided into three grades (1-3), with the functionality of each domain becoming more complex as the grade increases (NSW Ministry of Health 2017). Additionally, the role is often co-created by the needs of the employing organisation and the individuals within the role, rather than by the role domains captured in the position description (Jokiniemi et al. 2012). Despite differences in nomenclature, the role is similar to those of the United Kingdom's 'Nurse Consultant' and the United States' 'Clinical Nurse Specialist', who also experience similar issues around role enactments of their role descriptions (Jokiniemi et al. 2012). These roles all belong to a broader term of 'advanced practice roles', which have been,
'recognised and described as a level or practice rather than a role or a title'
(Dragon 2016)
CNC/CMCs provide a positive contribution both to their organisation and to patient outcomes (Bloomer & Cross 2011; Jannings & Armitage 2001; McIntyre et al. 2012; Philip et al. 2015; Roche et al. 2013; Walsh et al. 2015; Yacopetti et al. 2010). Often it is their high level of clinical knowledge, and their knowledge of how to work within the complexity of the health care system, that ensures the needs of patients, the health service, the team and the organisation are met (Walsh et al. 2015). Supporting the career and succession planning of these advanced nursing and midwifery roles would therefore benefit all stakeholders, including the LHD, the team, the current CNCs, those aspiring to the role and, most importantly, patients.
Eligibility for a CNC/CMC position requires the nurse/midwife to have between five to seven years' full-time post-registration experience, and experience in their specialty field. In addition, the employee must have an approved post-graduate nursing/midwifery qualification relevant to the field in which he/she is appointed, or other qualifications or experience deemed appropriate by the public hospital or public health organisation. An employer may also require a higher qualification in the specialist-nursing field, where such a qualification is considered essential for the performance of the individual position (Industrial Relations Commission of New South Wales 2017).
A number of studies have previously explored education preparation for the CNC/CMC role (Baldwin et al. 2013; Chiarella, Hardford & Lau 2007; Wilkes, Luck & O'Baugh 2015). Chiarella and colleagues (2007) found 10% of CNCs across New South Wales held no post-graduate qualification in their specialty, with one tertiary hospital finding as many as one third of CNCs not possessing post-registration graduate nursing qualifications (Roche et al. 2013). A gap has been identified in the literature regarding the contribution that education courses make to enhancing the CNC/CMC's knowledge and function in the five domains. Since every tertiary qualification comes at a financial and personal cost to the individual nurse/midwife, one objective for this research is to explore the contribution of education courses to the CNC/CMC practice domains.
Almost a decade ago, Burton, Bennett & Gibbon (2008) identified that succession planning for future UK consultants was neglected in policy development. In 2018 there remains a scarcity of literature on the subject. Planning for a future workforce is often difficult and, without adequate forward thinking, advanced nursing roles may not be replaced adequately in times of leave or resignation (Raftery 2013; Sprinks 2015). There is a need for LHDs to consider the costs of not implementing a strategic succession plan, rather than focussing on what strategic succession planning would cost (Hoffman & Womack 2011). According to Carriere and colleagues (2009), critical elements of a successful succession plan include: the development of a strategic plan outlining the organisation's objectives; the desired skills and individual needs of candidates who will support the strategic plan; adequate resource allocation; future development processes; and an inbuilt evaluation tool. Early identification and mentoring of successful candidates are also recommended. Reviewing these elements assisted the research team to consider topics for exploration in this study.
Career planning is defined as the continuous process of thinking about your interests, values, skills and preferences, exploring the life, work and learning options available to you, ensuring that your work fits with your personal circumstances, continuously fine-tuning your work and learning plans to help you manage the changes in your life and the world of work (Institute of Managers and Leaders 2018).
Succession planning and management focusses on identifying future leaders and preparing them for the role. It is a deliberate and systematic effort by an organisation to ensure leadership continuity in key positions, so as to retain and develop intellectual and knowledge capital for the future and to encourage individual advancement (Rothwell 2010).
This study was conducted to generate evidence to support the development of a local CNC/CMC Network career and succession planning strategy aimed at current and future CNC/CMCs. The objectives were to:
One hundred (n = 100) CNC/CMCs employed by this LHD were invited to participate in the study, including those in secondments and in temporary contracts.
A mixed methods approach was used, which combined both quantitative and qualitative data-collection methods within an electronic survey. Following the survey and its analysis, focus groups were held to explore the survey findings further.
This research received ethical approval from the joint University of Wollongong and the Local Health Districts Medical Human Research Ethics Committee (LNR 2017/144). Data collection began in March 2017 and was completed by June 2017. Approval to conduct this research project was provided by the research team's line managers.
Written participant information sheets outlining the overall details of the project were developed and forwarded by email to all CNC/CMCs within the Network. The project plans were discussed at CNC/CMC Network meetings, and all CNC/CMCs were invited to participate in the survey and/or the focus groups.
An electronic 20-minute survey was developed, tested, revised and then disseminated using eSurvey Creator™ (See Appendix 1: Example of survey questions). A blend of multiple-choice questions and free-text questions was used. The survey explored the following topics: demographics, education, and mentoring activity. To avoid ambiguity, the term 'education' was defined as,
'the process of receiving or giving systematic instruction, especially at a school or university, or a body of knowledge acquired while being educated, or information about or training in a particular subject'
(Oxford Dictionary)
and mentoring defined as,
'a senior professional (mentor) who invests and shares their time, effort, knowledge and expertise with a less experienced professional (mentee) to nurture their knowledge, skills and professional growth'
(Management Mentors 2018)
Demographics included: the respondent's age; years worked as a nurse; how they obtained initial registration; years in the CNC/CMC role; years in the specialty before gaining the position; employment status; years they anticipated continuing in the role; and full- or part-time status.
The education questions explored the respondent's education pathway before becoming a CNC/CMC, and how they believed this then linked to knowledge of the five domains of the CNC/CMC role. The same questions were repeated, focussing on the respondent's education pathway after becoming a CNC/CMC. Also investigated were the CNC/CMC's priorities for their future educational needs, and what they perceived an aspiring CNC/CMC should prioritise for their education.
Mentoring question explored the number of CNC/CMCs who had received mentoring prior to, and whilst in, the CNC/CMC role. It was deemed important to identify whether they were currently mentoring a potential successor into their role.
The CNC/CMC Network provided 100 prospective participants' names (including those CNC/CMCs in seconded positions). Their email addresses were entered into the survey system and they were sent an invitation to participate. The surveys were anonymous and participants were given the option to skip questions that they felt might potentially identify them. Using this survey system allowed three reminders to be sent, two weeks apart, to those who had not completed the survey, up until the close date. All participants were known to have computer and email access. Consent was implied by completion of the survey.
The survey platform, eSurvey, supported data analysis, as it developed an automatic report and a summary of quantitative results. This data is reported as descriptive statistics. The free text answers were themed by the research team. Information collected about the courses undertaken by the survey respondents also included their perceptions of how the course supported their knowledge in each of the five domains. The research team then reviewed the courses and categorised each into what they deemed to be that course's primary domain focus: e.g. a graduate certificate of leadership and management was placed in the leadership domain as its primary focus, whereas a graduate certificate in aged care was deemed to have a major clinical focus. Those with a broad remit, such as the Master's of Nursing (with no specialty assigned to them) were categorised as 'broad', and when the grade of the course was mentioned but no name given it was labelled 'unspecified'.
All CNC/CMCs were invited to participate in Part 2 (focus groups). Completing Part 1 (eSurvey) was not a pre-requisite. Attendance was voluntary. An expression of interest was sent to all CNC/CMC Network members twice by email, and one face-to-face invitation was announced at a CNC/CMC Network meeting. (This invitation to participate was minuted for those not in attendance.) Of the total CNC/CMC group, 19% attended one of the three focus groups.
A series of three face-to-face focus groups were conducted: Focus Group A (FGA) with nine participants; Focus Group B (FGB) with six participants; and Focus Group C (FGC) with four participants. The focus group format was developed following analysis of the survey results. It consisted of a PowerPoint presentation of the survey data findings, following which the participants were asked to give meaning to the results and further clarify any questions the researchers had about the results from the survey. The focus groups were held in two different locations and lasted approximately 90 minutes each. Written consent was required to participate in the focus group. The focus groups were led by one of the co-investigators with support from the lead investigator. During the focus groups, one investigator facilitated and one scribed notes to capture key points, which were then fed back to the participants for checking. The focus groups were also audio-recorded and the recordings were transcribed.
The qualitative data was analysed for themes using a thematical analysis process, an approach that can be used by those with less experience conducting qualitative research (Braun & Clarke 2014). Braun & Clarke (2006, p. 10) state that,
'through its theoretical freedom, thematic analysis provides a flexible and useful research tool, which can potentially provide a rich and detailed, yet complex account of data.'
All the researchers read the focus group transcriptions. The transcripts were then coded, categorised and themed. The themes were finalised when the research team were in agreement. No software was used; the coding was done manually and an audit trail was developed and saved as part of the research data.
This section combines both survey and focus group results under the following headings: Demographics (objective 1); Education preparation (objective 2); Education priorities (objective 3); and Mentoring (objective 4).
The survey was completed by 61% of the CNC/CMCs and 19% participated in the focus groups. Despite only three focus groups being held, each revealed common themes with very little variability, achieving data saturation. This study captures CNC/CMCs across a large geographical area consisting of both regional and rural services. There was good participation across all clinical streams and different CNC/CMC grades, with a variety of experience in the role.
Table 1 depicts the CNC/CMC Network as a very experienced workforce with a large majority (approximately 70%) of its members having 20 years' or more nursing/midwifery experience. Despite being clinically experienced, 44% of the CNC/CMCs have been in the role for four years or less. 44% percent of CNC/CMCs worked in their specialty for 5-9 years before obtaining the CNC/CMC role, whilst 39% worked in their specialty for 10 years or more before obtaining the role.
Almost three quarters of the participating CNC/CMCs work full time (74%) and 82% were in permanent positions.
As can be seen in Table 2, a large majority of CNC/CMCs (more than 80%) are aged 40 years or older and 1 in 12 are aged 60 years or more. Almost a quarter (24%) of the respondents reported that they intend to leave the role within 5 years, with a further loss of another 25% within the next decade.
Table 1: Demographic information
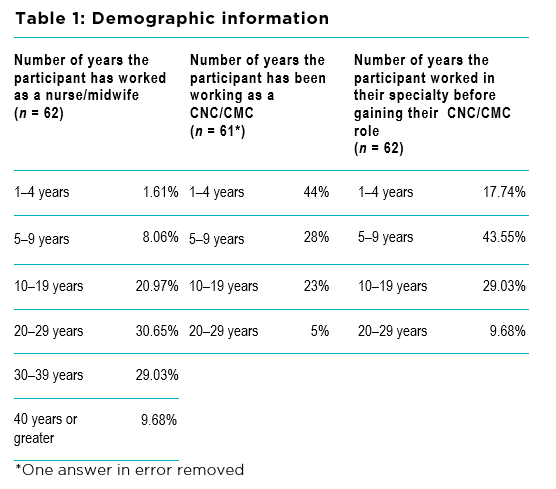
Table 2: Demographic information of CNC/CMCs by age and number of years continuing in the role
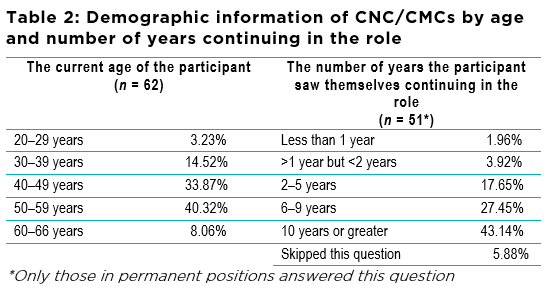
*Only those in permanent positions answered this question
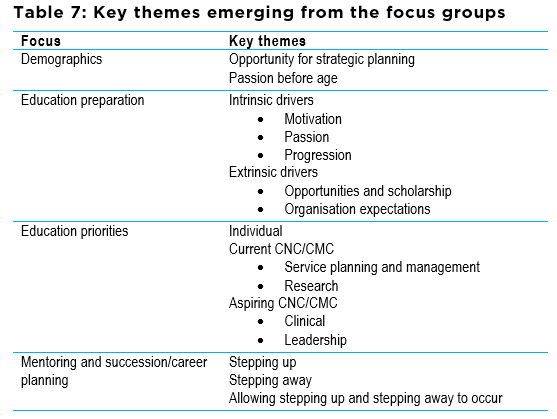
Two themes emerged within the focus groups in regards to the demographic data: 'opportunity for strategic planning' and 'passion before age'.
The focus-group participants felt that the likely loss of highly experienced nurses over the next decade can be explained by the age of the CNC/CMC Network members and future retirements. This was seen as an opportunity for strategic planning by the CNC/CMC Network in collaboration with the LHD Nursing and Midwifery Executive, to support current CNC/CMCs and persons aspiring to the role. However, consideration needs to be given to the current pool of nurses from which new CNC/CMCs will be drawn, and thus mentoring will become an imperative. The participants also urged the LHD to offer greater flexibility in working hours in order to retain the current highly skilled and experienced nurses/midwives, with part-time working an option that many CNC/CMCs would take.
Some focus-group participants expressed the view that age should not be seen as an indicator of experience or ability, and should not be seen as a pre-requisite to becoming a CNC/CMC. The word 'passion' was used to describe the attribute required of the aspiring CNC/CMC:
'It's when you show that passion and interest, and you learn every day about the subject and you're questioning and making changes at your ward level'
(FGA)
Table 3 indicates that 55% of CNC/CMCs were university trained. Over 90% have obtained a graduate certificate or greater as their highest level of education since registering as a nurse/midwife. The 6.45% who chose the 'other' category as the highest level of education were those who obtained Bachelor degrees and one specialty course, which was equivalent to a Master's level. A small number (n = 2) had 'specialist course' as their highest level of education, which was defined as courses over two days in duration but not at graduate level. The participants were asked to select their highest level of qualification; 35% chose a Master's degree. However, in the dataset a further eight Master's were found and we can only assume these were courses in progress, which could adjust the percentage of CNC/CMCs either working towards or having obtained a Master's degree or above from 39% to 47%. This would include the two CNCs who each had a PhD and three Master's courses between them.
The 62 participants were broadly educated, having undertaken an additional 142 education courses (Table 4). Some had completed more than one course. The majority of CNC/CMCs had undertaken further education prior to becoming a CNC (n = 88 courses), of which 66 courses were at a post-graduate level. Of the courses taken prior to the role, only 32% ( n = 27) were completed with the aim of working toward the CNC/CMC role. Approximately two thirds of those who held a Master's level qualification obtained this before becoming a CNC/CMC.
CNC/CMCs who had been in the role for 10 years or less undertook 70% of all Master's courses.
Table 3: Initial registration and highest level of education
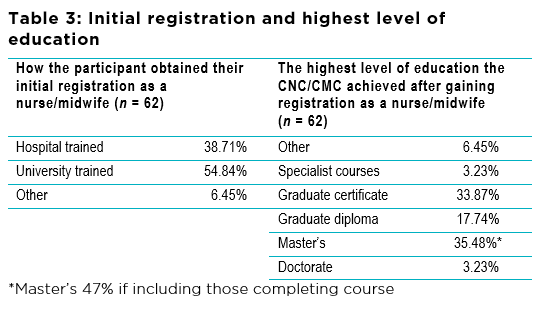
Table 4: Level of courses taken by CNC/CMC participants prior to and while in the role, and the researchers' opinion of the courses' primary domain

Table 4 shows that, of the 88 courses undertaken prior to the CNC/CMC being in the role, 44% (42/88) primarily focussed on a clinical specialty and 15% (13/88) focussed primarily on education. Over half of the CNC/CMCs continued to undertake further education courses while in the CNC/CMC position (n = 54 courses), of which 44% focussed primarily on a clinical specialty and 30% on leadership. Only one participant undertook a course with a primary focus on service planning and management.
Only 11% of graduate certificates and 37% of Master's courses were reported to increase the participant's knowledge across all five domains.
The focus groups identified intrinsic and extrinsic factors that motivated participants to pursue further education. Three sub-themes emerged from the intrinsic drivers: personal motivation, passion, and progression of career. The influence of the LHD was an extrinsic driver.
Personal motivation to learn more about the subject or specialty prior to the role was seen as a key intrinsic driver. CNC/CMCs believed that personal drive and an interest in the subject motivated them to study and to develop professionally. These courses were often not undertaken specifically to gain the CNC/CMC role, but they often helped when applying for a position.
Passion is the personal drive to improve care or service for better patient outcomes. The participants believed that passion for their work was vital to the delivery of better service and improved patient experiences and outcomes. Passion often drives the pursuit of specialty education.
'The passion drives the piece of paper'
(FGA)
Education choices become more purposeful once in the CNC/CMC role, as education enhances the knowledge and functionality within the role. Knowledge is also acquired through various modalities other than formal studies, such as: attending conferences, reading journals, and being part of specialty working parties and research.
Progression of career is the personal motivation and self-improvement required to obtain and perform the role well. Education was thought to provide access to better job opportunities and to progress their careers:
'I did my Masters to make sure I got the job.'
(FGA)
The participants also believed that education gives a good foundation to better functioning within their role. Focus-group participants with a Master's level of education overwhelmingly stated that it helps them meet the CNC/CMC domains. There was disagreement in regards to the timing of that Master's level of study. Some participants stating that it should be undertaken prior to commencing the CNC/CMC role in order to better prepare for work across the domains, while others felt a specialty qualification would help them to progress into the role, and then the Master's course could be more tailored to the CNC/CMC's specialty and needs.
'If I went into another role without that formal training with the Master's I would have a lot of trouble… it really made a huge difference.'
(FGC)
Some participants had experienced managerial support to pursue further education through encouragement to apply for scholarships, while others felt that further education was expected of them in order to enhance their knowledge and skills within the five domains. The participants remarked on the cost of education and suggested that the LHD could consider some form of education scholarship. Additionally, the current industrial agreement does not support the payment of an education allowance for CNC/CMCs, but does for those employed at a lower clinical level.
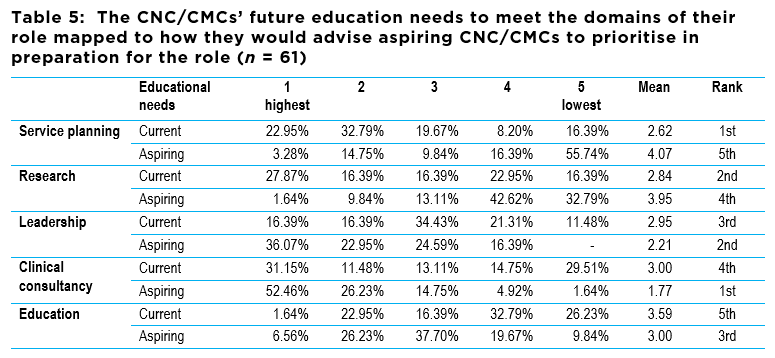
Table 5 indicates the survey participants' responses regarding prioritising their own education needs in relation to the five CNC/CMC practice domains (clinical services and consultancy; clinical leadership; research; education; and clinical service planning and management). The scoring ranged from 1 = highest priority to 5 = lowest priority, with their mean scores ranging from 2.62-3.59. Service planning and management was the top priority, with a mean score of 2.62, followed closely by research (mean score 2.84).
The CNC/CMCs were also asked to rank the domains that an aspiring CNC/CMC should focus their development on. These results were in almost reverse order, with the clinical service and consultancy domain being the key priority (mean 1.77) followed by clinical leadership (mean score 2.21), with service planning and management deemed the last priority (mean score 4.07). The scores for the aspiring CNC/CMCs were spread across a greater mean range than were the current CNC/CMCs' priorities (mean scores range 1.77-4.07).
Despite the overall education priorities captured by the survey, the focus-group participants highlighted that there also needs to be consideration of the individual CNC/CMC's education needs. These needs were explained by each CNC/CMC's role being unique: the work contexts differ, there is a range of CNC/CMC job descriptions, and different individual nurse/midwives bring different previous experiences, knowledge and education to the role. Clinical Nurse/Midwifery Specialists were discussed as these staff often step
Table 5: The CNC/CMCs' future education needs to meet the domains of their role mapped to how they would advise aspiring CNC/CMCs to prioritise in preparation for the role (n = 61)
up to the CNC/CMC role and should have leadership, education and consultancy skills. These individuals would require support with the other domains to make the transition.
The CNC/CMCs' choice of clinical service planning and management as their highest priority for future education needs is explained by a lack of specific education available for this domain. There were avenues to gain education in the other four practice domains. The participants explained why research was the second priority within the survey, identifying that they do not possess enough knowledge in this area and that it is something they would like to achieve:
'If you do research, you understand evidence-based practice… which helps you with transferability and translation into practice"
(FGB)
However, this priority was also prompted by the Chief Executive Officer's expectations regarding research output from CNC/CMCs.
Clinical service and consultancy knowledge was recognised as a strong requirement for the CNC/CMC, due to the autonomy of the role and the need to be clinical experts in their specialty. being seen as clinical experts. For some current CNC/CMCs this was a priority for their own education, but less so for others. The focus-group participants did not identify any specific reasons why education was ranked as the lowest priority for themselves.
The participants overwhelmingly ranked the clinical consultancy domain as the highest education priority for aspiring CNC/CMCs, explained by the need to ensure that they are safe and knowledgeable clinicians. Leadership was also acknowledged as an essential skill to be an effective CNC/CMC:
'If you are a good leader then the results will follow'
and this happens because you
'can smooth the way and stand up for what you think and be recognised in that position'
(FGA)
Table 6 shows that only one in five CNC/CMCs were currently involved in mentoring aspiring CNC/CMCs. There was a greater number of CNC/CMCs mentored while in the CNC/CMC position than those who had experienced mentoring prior to holding the position (57% versus 34%).
In the focus groups, succession and career planning were seen as everyone's responsibility: the aspiring CNC/CMC and the CNC/CMCs within the position, and the LHD. The interplay between these groups would allow the aspiring CNC/CMC to 'step up' into the role and trial the position in a supported way, whilst the LHD supports the CNC/CMC to 'step away' from their position. A range of barriers have been identified for mentoring others into the role. These will be discussed below.
Table 6: Mentoring activity
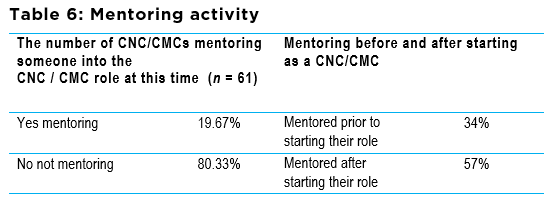
Table 7: Key themes emerging from the focus groups
The participants identified that aspiring CNC/CMCs need: to be passionate about their specialty; be clinically experienced; be valued by others; have a commitment to lifelong learning; be educated to a specific level; and have patience.
The survey indicated that more than 40% of roles may not be vacant for ten years or longer; however, many participants described how some new roles just transpired and they were then under prepared for the transition into the role. An aspiring CNC/CMC needs to be proactive in expressing their desire for the role so that, when the role becomes available, they are already potentially being considered for it. As one participant stated,
'I think you'll find that nearly every CNC if you ask them, will probably say they've had a tap on the shoulder to say that they would be a good candidate for it (the role) to throw their hat in the ring.'
(FGA)
To prepare and support aspiring CNC/CMCs, mentors need to be sought who can assist them in identifying their strengths and explore how best to invest their time.
Some participants identified a number of educational initiatives they already provide to aspiring CNC/CMCs, such as supporting their access to formal education programs, providing learning packages, and encouraging them to apply for conference funding. There were also experiential learning opportunities for the aspiring CNC/CMC. These included: opportunities to work with current CNC/CMCs on collaborative projects; taking aspiring staff to meetings; and encouraging networking opportunities, both internal and external to the LHD. This relationship allowed the aspiring CNC/CMC to be exposed to the larger health arena as one clinical nurse consultant explained:
'they [the aspiring CNC/CMCs] need support for challenging situations rather than fend for self. How do you voice for your service? What do these behaviours look like? Role model… I learned from another CNC you have to be involved in your bigger LHD…. You need to get involved with a professional group.'
(FGA)
Many CNC/CMCs were not ready to step away from their role as they perceived many benefits to it, such as,
'maintaining clinical contact with people and patients'
(FGB)
and less shift work. However, being able to step away from the role for either short-term or permanent leave required the CNC/CMC to be organised, and to ensure adequate internal and external support for their replacement. Some were unsure of where to start with succession planning, but there was an awareness of needing to be proactive, no matter what stage you were at in your CNC/CMC role.
A number of barriers to stepping away affected succession planning and mentoring:
The focus-group participants offered a range of strategies to support career and succession planning However, there was a sense that it is all in the
'too hard basket'
(FGA)
causing frustration amongst some of the participants. This frustration was directed towards the aspiring CNC/CMCs not being supported to step up to the participant's roles during times of CNC/CMC leave. To facilitate stepping up, the participants suggested the following:
'I was at a CNC meeting…and they were talking about succession planning, they were all talking about who would take their places while they are on leave and I said to them, "Excuse me, I'm in this room and you're not even mentioning my name and you're not giving anybody an opportunity to go for these jobs."'
(FGB)
There was a dissonance between the LHD and the CNC/CMCs in regards to the education requirements for those covering leave provisions. Often, specialty education is a pre-requisite for applying for a secondment CNC/CMC role, which significantly reduces the number of potential applicants. The CNC/CMCs themselves would prefer someone in their role with clinical expertise, rather than educational qualifications. For some, stepping into the CNC/CMC role for leave provision sent them on an education pathway to ensure that they secured the position when it became available in the future.
The aim of this research was to generate evidence to support a local career and succession planning strategy for current and future CNC/CMCs. To meet this aim, current CNC/CMCs were invited to share: their demographics, their education pathways, their education needs; their perceptions of the education needs of aspiring CNC/CMCs; and their mentoring experience. The findings of this research can support future thinking for managers, current staff and aspiring CNC/CMCs, as succession and career planning was deemed to be everybody's business. Recommendations have been integrated into this discussion.
These findings confirmed that CNC/CMC Network members' concerns about their own ageing workforce were warranted. Nearly 50% of the cohort were 50 years old or older; this is consistent with others' findings (Chiarelli, Hardford & Lau 2007; Wilkes, Luck & O'Baugh 2015). The knowledge that a high percentage (24%) of CNC/CMCs intend leaving within five years, with a further expected loss within ten years, provides evidence that a CNC/CMC succession planning strategy is required now. The release of a local nursing and midwifery workforce plan confirms that this district has 'leadership' succession planning on its agenda and is making a systematic effort to ensure leadership continuity. As important clinical leaders, the CNC/CMCs need to ensure that they are seen as part of the succession planning strategy as it is currently aimed at managers. Otherwise, the LHD will risk losing the knowledge and skills of highly experienced clinical leaders without prior transference of these skills and knowledge to others. For those aspiring to the role of a particular CNC/CMC specialty, it would be worth investigating the intention of the current role holder, as 50% of CNC/CMC positions will not be available for ten years or longer and this may influence career choice and educational preparation for future roles.
This study provides additional areas for nursing and midwifery leaders to consider within a succession planning strategy: flexible work practices; ongoing supports; and experiential learning opportunities. Within this LHD almost 35% of the nursing workforce works part time, in comparison to 25% of CNC/CMCs (Illawarra Shoalhaven Local Health District, Nursing and Midwifery 2016). Within the focus groups, many participants indicated that they would be prepared to work part time to allow for succession planning to occur. These flexible work practices have the potential to provide a supportive environment for a CNC/CMC's transition period. Supportive environments have been recognised as a key requirement for the nurse to function in newly developed advanced roles (Hourahane et al. 2012). This study also identified that some CNC/CMCs felt a lack of support in their role. In their systematic review of Australian advanced nursing practice roles within acute settings, Ramis, Pearson & Wu (2013) found a lack of professional support and professional isolation and recommended supports to avoid the risk of burnout due to the demands of the advance practice nursing roles. Therefore, ongoing support of new and established CNC/CMCs must be an integral part of succession planning or career planning, rather than something that ceases on their entering the role.
A successful succession plan requires resources (Carriere et al. 2009). The CNC/CMCs expressed the importance of 'backfilling' their roles and allowing others time in the position to support experiential learning. Leave provision does not occur consistently across divisions and departments and requires planning at a strategic level. The issue of backfill for these roles is not unique to this LHD (Bloomer & Cross 2011), or to CNCs - Nurse Practitioners share the same issues (Raftery 2013). A partnership between the nursing and midwifery executive and the CNC/CMC Network could negotiate time for aspiring CNC/CMCs to learn the role in different ways, being mindful of today's economic climate. Backfilling roles requires mentoring beforehand.
Mentoring is a form of positive support where an experienced and a less experienced professional work together to help the mentee to reach their full potential and to develop their career. In their integrated literature review, Carriere and colleagues (2009) found mentoring to be an important factor in successful succession planning. A proactive approach to identifying potential candidates is recommended to provide a resource when a gap occurs. At this time, only 20% of CNC/CMCs are formally mentoring someone into their role; this does not match the number of staff intending to leave their position. This research provides evidence to review and revive a current LHD mentoring program. However, it is important to acknowledge that the question was in relation to formal mentoring and it has been shown that mentoring can occur informally by nurses, 'simply doing their job during the normal course of the day' (Thomka 2007, p. 23). Thomka interviewed nurses who described relationships of an informal nature, formed over time due to the proximity of working together, resulting in knowledge sharing. This is achieved through teaching, role modelling and leading patient care. Mentorship is not just for those aspiring to or new to the role, it has also been proposed that advanced practice nurses consider longer term mentorship with a range of multiple mentors, as their needs change over time (Doerksen 2010; Franks & Howarth 2012). Finding ongoing mentors for CNC/CMCs would serve three functions: to provide ongoing support (Ramis, Pearson & Wu 2013); to help them with domains such as service planning and management (an area that the study found was not covered by many educational courses); and to role model how mentoring should occur so the CNC/CMCs can then emulate the process with aspiring CNC/CMCs.
Identifying common education paths taken by the CNC/CMCs prior to the role, and exploring how they perceive this education has supported them to meet the domains of CNC/CMC practice, has the potential to support aspiring CNC/CMCs in decision-making and career planning for their future. The current literature only reports the highest qualifications that CNC/CMCs have achieved, with no reports on the relationship of these courses to the CNC/CMC practice domains (Chiarella, Hardford & Lau 2007; Baldwin et al. 2013; Wilkes, Luck & O'Baugh 2015). This study found only 11% of post-graduate certificates were perceived to provide knowledge across all five domains, in comparison to 37% percent of all Master's level qualifications. Despite the small sample size, this is an important finding and warrants further exploration in a larger study. The minimum current recommendation for incoming CNC/CMCs' education preparation is a post-graduate qualification in their specialty. A larger study would determine the minimum level of qualification to support the CNC/CMC to have the knowledge to fully function in the role. However, the contribution the Master's course provides to fully function in the role was also verified in the focus groups.
This study found that a myriad of different courses and education pathways were undertaken prior to the CNC/CMC role, which may partly be due to the fact that the courses were not in preparation for the role. This study also found that different job descriptions, work contexts, and the individual nurse/midwives' previous experiences, knowledge and education also impact current and future education. The organisation's needs are known to affect how the advance nursing roles are enacted (Jokiniemi et al. 2012), but these organisation needs also play a role in the education undertaken by the CNC/CMCs. Using the five domains of practice in career planning or performance appraisal would support the ongoing development of aspiring and current CNC/CMCs and may provide some form of uniformity in the enactment of the role in line with the industrial award. Incorporating the principles of adult learning would allow the CNC/CMC to take the lead in their education needs, with a commitment to gain knowledge in all five domains.
This study found that 65% of CNC/CMCs who obtained their Master's qualification did so before being in the role. This indicates that, despite the minimum entry level being a graduate qualification, aspiring CNC/CMCs are preparing themselves to a higher Master's level and, according to the CNC/CMCs interviewed, they are thus better prepared to work across the role domains. A Master's level is recommended in the UK for Nurse Consultants (a similar role to that of CNC) (East et al, 2015). Other UK studies have found that a Master's level qualification and previous engagement with research (along with the nurses' attributes and nursing experience) support Nurse Consultants with the requirements of the role (Woodward, Webb & Prowse, 2005; Burton, Bennett & Gibbon. 2009). It has also been proposed that higher degrees in the clinical specialty may not necessarily be required; preparation in research or leadership may be more beneficial, as the nurse is already an established clinician before obtaining the role (Franks & Howarth 2012). Considering the cost of post-graduate courses, it is important for aspiring CNC/CMCs to review the education courses they are considering and how they align to the five CNC/CMC practice domains. It may also be relevant to those who are employing or mentoring future CNC/CMCs to consider the CNC/CMC's strengths in the domains and areas where development can be focussed. Each workplace also provides rich sources of learning - formally and informally - that should not be discounted in favour of purely academic courses.
The current CNC/CMCs, many of whom did not proactively chose their education with a view to the CNC/CMC role, encourage aspiring CNC/CMCs to concentrate their future development upon two clear domains: clinical consultancy and leadership. This is not surprising as many CNC/CMCs function in the clinical service and consultancy domain at the expense of the other domains (Roche et al. 2013). Walsh and colleagues (2015), in their qualitative study looking at how CNC roles were viewed in this LHD, found the clinical and leadership domains to be interlinked, as being professionally credible allows the CNC/CMC to achieve leadership and work with others. Although CNC/CMCs function at the clinical interface, for the role to be successful they must influence both at the clinical and at the organisational level, which requires leadership development (Hourahane et al. 2012).
Career planning also applies to the nurse/midwife in the role and their ongoing learning needs. There was a reduction in formal education courses taken after being employed in the role, but learning continues through different modes: attending conferences; reading journals; participating in research and quality improvement activities; and receiving mentorship. A UK study reported that non-medical consultants found conferences provided them with more currency than academic courses did (Burton, Bennet & Gibbon 2009). This study found most courses provided no knowledge of the service planning and management domain, which explains the expressed education need of the current CNC/CMCs. This research did not identify a solution to this problem, but it is one that needs to be considered at a local level as part of the career and succession planning strategy as it is not being provided by the academic organisations. This is a domain where executive leaders with service planning and management skills could support clinical leaders to increase their knowledge.
'Research' was the second highest education priority of the current CNC/CMCs. The vision of the Chief Executive Officer had a 'flow through' effect, with many managers asking for research outputs from the CNC/CMCs, indicating the contextual and LHD influence on the enactment of the CNC/CMC practice domains (Jokiniemi et al. 2012; Wilkes et al. 2015). Research has been reported as being difficult for advanced practice nurses, despite it being a key expectation of the role. There are a range of reasons behind this: the time for conducting research is often lacking (Bloomer & Cross 2011), whilst some CNC/CMCs perceive that it should not be a frequent part of their role (Wilkes, Luck & O'Baugh 2015), and others see it as an extra task (Cashin et al. 2015). However, a more recently published study of Australian advanced practice nurses (including the CNC/CMC), found that these roles scored significantly higher at the advanced practice levels in the areas of research and professional leadership than did specialist and registered nurses (Gardner et al. 2017). In this LHD, the CEO has provided ongoing support to nurses and midwives through the appointment of a Professor of Nursing and Midwifery Research. This position provides an internal research resource for all nurses and midwives and, in other LHDs, working with academic staff has proven to have a positive effect (Gallagher et al. 2013). Again, a research mentor could support aspiring CNC/CMCS.
These results may not be generalisable to the metropolitan hospitals or other LHDs as this is a regional and rural District Health Service. The number of Master's degrees taken was too small to make vast inferences about their ability to support knowledge across all domains. However, further study in this area may be warranted. In particular, are the current education criteria for a CNC/CMC within the NSW Health Service adequate to support the nurses/midwives to perform their roles across the five domains?
Given the opportunity to redo this research, the researchers would more thoroughly investigate the role that mentoring plays in developing aspiring CNC/CMCs and whether the current CNC/CMCs were seeking mentoring themselves towards individual CNC/CMC domains.
The intellectual capital and practice wisdom of many CNC/CMCs will be lost over the next decade if a succession and career planning strategy is not put in place within this LHD. A number of areas were identified for nursing and midwifery leaders to explore within their succession and career planning strategy, such as flexible work practices, support mechanisms (including mentoring for aspiring and current CNC/CMCs), and providing experiential learning opportunities.
Despite being a local project with a relatively small sample size, some findings may be of interest to other LHDs and areas and warrant further research. The CNC/CMC role spans five practice domains and, from our findings, few courses provide knowledge across them all. This raises the questions: how can a CNC/CMC prepare for the breadth of the role; and what can an organisation do to support them in their role? Master's courses performed better than graduate certificates, but the numbers of courses were too small to make large inferences. Few courses provide support in the service planning and management domain, which was seen as the priority area of education need for many CNC/CMCs. Aspiring CNC/CMCs are advised to develop their consultancy skills and clinical knowledge and their leadership skills and should also explore education courses to ensure a return on their financial investment.
The authors would like to acknowledge the CNC/CMC Network group and the Nurse Managers who supported the research group.
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
No funding was received for this project.
Baldwin, R, Duffield, C, Fry, M, Roche, M, Stasa, H & Solma, A 2013, 'The role and functions of Clinical Nurse Consultants, an Australian advanced practice role: A descriptive exploratory cohort study', International Journal of Nursing Studies, vol. 50, pp. 326-334.
Bloomer, M & Cross, W 2011, 'An exploration of the role and scope of the Clinical Nurse Consultant (CNC) in a metropolitan health service', Collegian, vol. 18, pp. 61-69.
Braun, V & Clarke, V 2006, 'Using thematic analysis in psychology', Qualitative research in Psychology, vol. 3, pp. 77-101.
Braun, V & Clarke, V 2014, 'What can "thematic analysis" offer health and wellbeing researchers?' , International Journal of Qualitative Studies on Health and Well-being , vol 9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4201665/
Burton, CR, Bennett, B & Gibbon, B 2009, 'Embedding nurse and therapy consultantship; the case of the stroke consultant', Journal of Clinical Nursing, vol. 18, pp. 246-254.
Carriere, B, Muise, M, Cummings, G & Newburn-Cook, C 2009, 'Healthcare succession planning - an integrated review', The Journal of Nursing Administration, vol. 39, pp. 548-555.
Cashin, A, Stasa, H, Gullick, J, Conway, R & Buckley, T 2015, 'Clarifying Clinical Nurse Consultant work in Australia: A phenomenological study', Collegian, vol. 22, pp. 405-412.
Chiarella, M, Hardford, E & Lau, C 2007, 'Report on the evaluation of Nurse/Midwife Practitioner and Clinical Nurse/Midwife Consultant Roles', NSW Department of Health, N Sydney.
Doerksen, K 2010, 'What are the professional development and mentorship needs of advanced practice nurses?', Journal of Professional Nursing, vol. 26, pp. 141-151.
Dragon, N 2016, 'Advanced Nursing Practice - A level in its own right.' Australian Nursing and Midwifery Federation, vol. 24. Viewed 20 June 2018 http://anmf.org.au/featured-stories/entry/advanced-practice-nursing-a-level-in-its-own-right
East, L, Knowles, K, Pettman, M & Fisher, L 2015, 'Advanced level nursing in England: organisational challenges and opportunities', Journal of Nursing Management, Vol 23, pp. 1011-1019.
Franks, H & Howarth, M 2012, 'Daring to be different: A qualitative study exploring the education needs of the nurse consultant', Nurse Education Today, vol. 32, pp. 406-411.
Gallagher,R , Sadler, L, Kirkness, A, Belshaw, J, Roach, K & Warrington, D 2013, Collaboration: a solution to the challenge of conducting nursing research in cardiac rehabilitation. Collegian (Royal College of Nursing, Australia) vol. 20, pp. 255-9.
Gardner, G, Duffield, C, Doubrovsky, A & Adams, M 2017, 'The structure of nursing; a national examination of titles and practice profiles', International Nursing Review, vol. 64, pp. 233-241.
Hoffman, T & Womack, S 2011, 'Succession planning: What is the cost of doing it poorly...or not at all?', Viewed 28th February 2018 https://www.pwc.com/gx/en/oil-gas-energy/publications/pdfs/energy-company-succession-planning.pdf .
Hourahane, G, West, N, Barnes, R, Rees, S, Bowyer, A, Dundon, J & Allen, D 2012, 'Supporting trail-blazing: A systematic review of the factors that facilitate or inhibit the implementation of new nursing roles: the experience of UK consultants nurses', JBI Library of Systematic Reviews, vol. 10, pp. 3146-3294.
Industrial Relations Commission of New South Wales 2017, Public Health System Nurses' and Midwives' (State) Award. Viewed 20 November 2018 https://www.health.nsw.gov.au/careers/conditions/awards/nurses.pdf
Institute of Managers and Leaders 2018, 'Member Exchange - Career Planning' [Accessed 15th February 2018]. https://managersandleaders.com.au/member-exchange-career-planning/
Jannings, W & Armitage, S 2001, 'Informal Education; A hidden element of Clinical Nurse Consultant Practice', The Journal of Continuing Education, vol. 32, pp. 54-59.
Jokiniemi, K, Pietila, A-M, Kylma, J & Haatainen, K 2012, 'Advanced nursing roles: A systematic review', Nursing and Health Sciences, vol. 14, pp. 421-431.
Illawarra Shoalhaven Local Health District, Nursing and Midwifery 2016, ISLHD Nursing and Midwifery Workforce Plan .
Management Mentors 2018, Definition of mentoring, benefits of mentoring, & other FAQs, retrieved 27 February 2018, https://www.management-mentors.com/resources/corporate-mentoring-programs-resources-faqs#Q1
McIntyre, T, Taylor, C, Eastwood, G, Jones, D, Baldwin, I & Bellomo, R 2012, 'A survey of ward nurses attitudes to the Intensive Care Nurse Consultant service in a teaching hospital', Australian Critical Care, vol. 25, pp. 100-109.
NSW Ministry Of Health 2017, Clinical Nurse/Midwife Consultants - List of domains and functions, retrieved 18 November 2018, https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/IB2017_002.pdf
Oxford Dictionary. Definition of Education in English, retrieved February 2018 https://en.oxforddictionaries.com/definition/education
Philip, S, Carter, J, Barnett, C, D'Abrew, N, Pather, S & White, K 2015, 'Patients' Perspectives of Fast-Track Surgery and the Role of the Fast-Track Clinical Nurse Consultant in Gynecological Oncology', Holistic Nursing Practice, vol. 29, pp. 158-166.
Raftery, C 2013, 'Nurse practitioner succession planning: forward thinking or just an after-thought?' Australian Health Review, vol. 37, pp. 585-587.
Ramis, M, Pearson, A & Wu, C 2013, 'The experience of being an advanced practice nurse in Australian acute care settings: A systematic review of qualitative evidence', JBI Database of Systematic Reviews and Implementation Reports, vol. 10, pp. 3960-4018.
Roche, M, Duffield, C, Wise, S, Baldwin, R, Fry, M & Solman, A 2013, 'Domains of practice and Advanced Practice Nursing in Australia', Nursing and Health Sciences, vol. 15, pp. 497-503.
Rothwell, W 2010, Effective Succession Planning - Ensuring Leadership Continuity and Building Talent from Within , American Management Association, New York.
Sprinks, J 2015, 'Could valuable leadership role be in danger of vanishing?', Cancer Nursing Practice, vol. 14, pp. 8-9.
Thomka, L 2007, 'Mentoring and its impact on intellectual capital - through the eyes of the mentee', Nursing Administration Quarterley, vol. 31, pp. 22-26.
Walsh, K, Bothe, J, Edgar, D, Beaven, G, Burgess, B, Dickson, V, Dunn, S, Horning, L, Jensen, J, Kandl, B, Nonu, M, Owen, F & Moss, C 2015, 'Investigating the role of Clinical Nurse Consultants in one health district from multiple stakeholder perspectives: a cooperative inquiry'. Contemporary Nurse, vol. 51, pp. 171-187.
Wilkes, L, Luck, L & O'Baugh, J 2015, 'The role of a clinical nurse consultant in an Australian Health District: a quantitative survey', BMC Nursing, vol. 14, pp. 14-25.
Woodward, V, Webb, C & Prowse, M 2005. 'Nurse consultants: their characteristics and achievements', Journal of Clinical Nursing, vol. 14, pp. 845-854.
Yacopetti, N, Alexandrou, E, Spencer, T, Frost, S, Davidson, P, O'sullivan, G & Hillman, K 2010, 'Central venous catheter insertion by a clinical nurse consultant or anaesthetic medical staff: a single-centre observational study', Critical Care and Resuscitation, vol. 12, pp. 90-95.
Mentor definition: A senior professional (mentor) invests and shares their time, effort, knowledge and expertise with a less experienced professional (mentee) to nurture their knowledge, skills and professionals
· What clinical division do you belong to?
· How many years have you worked as a nurse?
· How did you obtain your initial registration as a nurse?
· How many years have you been in the CNC/CMC role?
· How many years did you work in the speciality before gaining your CNC/CMC role?
· How many years do you see yourself continuing in the role?
· Are you working full or part time?
· How many hours do you work if P/T?
· What is the highest level of education you have achieved following registration as a nurse?
· Did you take any course PRIOR to becoming a CNC/CMC?
· What course did you take? Name course, level of course, duration, was it taken towards a CNC/CMC role? Please identify if you felt these studies prepared you for any of the CNC/CMC domains? (repeated x 13)
· Did you take any course AFTER becoming a CNC/CMC?
· What course did you take? Name course, level of course, duration, was it taken towards a CNC/CMC role? Please identify if you felt these studies prepared you for any of the CNC/CMC domains? (repeated x 13)
· As a CNC/CMC rank the domains in order of priority that you think requires more education in order for you to meet the needs of your role?
· Prior to becoming a CNC/CMC did you have a formal or informal mentor to support your career development?
· After becoming a CNC/CMC did you have formal mentoring to support your CNC/CMC role development?
· If you were to mentor an aspiring CNC/CMC rank in order of priority which domains you think they should focus their development on?
· Are you currently mentoring anyone to the CNC/CMC role?